
Covid is treatable! Too few people know that
Paxlovid is absurdly under-covered, leading to needless deaths

UPDATE: In July, the FDA authorized pharmacists to prescribe this drug, so, if you need the drug, you may now have luck simply doing that and citing any risk factor (which are described below, and which are very expansive.)
Treatment is still important, because more Covid waves are likely
Covid deaths are currently really low in the US:

But because immunity wanes in its protection, we should expect still further waves (though there’s no need for them to upend daily life.)
To get a sense of the near future, one can look to the UK, which currently has 100-200 Covid deaths a day, after getting a second wave of Omicron thanks to the “BA.2” Omicron variant:

A similar trend is likely in the US, as it usually lags the UK by a month or two. The winter will also likely bring a yet-bigger wave.
Also, despite the UK’s second Omicron wave, seen in the graphs, the country remains totally free of restrictions on daily life and travel.
That’s the right decision. But a couple hundred Covid deaths every day is — while not apocalyptically bad — still something we’d like to bring closer to zero.
We have an effective treatment for Covid! Paxlovid. It is massively underused
Fortunately, we DO have a way to reduce deaths even further. The ridiculously-underreported drug Paxlovid reduces hospitalization and death by 89% — if taken within 5 days of the start of symptoms (you’re not supposed to wait until you’re hospitalized to take it.)
The drug works by blocking an enzyme that the coronavirus needs to replicate on a very basic level — and as a result, is considered effective against all variants.
The drug’s effectiveness was determined in fall 2021, but regulations and production delays caused it to not be very available during the peak of the Omicron surge — during which 200,000 Americans died of Covid.
Fortunately, for a couple of months now, the pills have been in-stock at pharmacies all over the US: https://covid-19-therapeutics-locator-dhhs.hub.arcgis.com/
Unfortunately, even in the later part of the omicron surge, when the drug began to become available, Paxlovid doses largely just sat on pharmacy shelves, barely touched. Less than half of the supply ordered so far has been used. NPR reports:
… hundreds of thousands of courses of Paxlovid, a highly effective pill that cuts the risk of getting hospitalized with COVID by nearly 90%, are gathering dust on pharmacy shelves … less than half of the distributed courses have been reported as used.
HHS's Eisnor, speaking to health care providers in mid March, said he was troubled by reports that some pharmacies had asked if they could trash their remaining supplies of unexpired COVID pills.
… "I had a situation last week where a young person who ... got COVID called their physician for Paxlovid and was denied," says Tien [an infectious disease physician at University of California]: The patient had a risk factor for COVID, but their doctor did not think they qualified for the drug, based on age and vaccination status. "There are some people who want it and are being turned away, and then there are others who perfectly fit the criteria and don't want it," Tien observes.
Why sitting on shelves? Reason 1: Red Tape
A big reason Paxlovid is under-used is that you can’t just go a pharmacy and get Paxlovid. You need:
1. A positive Covid test (that’s reasonable enough)
2. You must be considered at high-risk of developing severe Covid
3. You must get a prescription from a doctor.
The UK also has similar over-regulation.
American authorities, fortunately, realized that the above requirements might too burdensome for many people — so President Biden, in his State of the Union speech months ago, promised:
… we’re launching the “Test to Treat” initiative so people can get tested at a pharmacy, and if they’re positive, receive antiviral pills on the spot at no cost.
Unfortunately, in practice, “Test to Treat” has been implemented about as competently as the similarly-named “Test and Trace” — which is to say, hardly at all.
Very few places have set it up, because not many have both testing ability and prescribing doctors readily available on site. In the whole state of Vermont, for example, there is only one clinic that is set up to “Test to Treat.”
But even many clinics that officially offer “test and treat” — actually don’t.
An Axios reporter caught Covid, and, in late March:
after hours on hold with 10 "participating" stores, I found that most had never heard of Test to Treat or were not yet offering it.
Whoops. Still, there is some hope that the government will have things together in time for the next winter surge.
Also, if a person is super informed about Covid, knows about Paxlovid, and knows that it should be taken within 5 days, they should be able to get good treatment now.
They can get a test, and then contact a doctor. Fortunately, the list of things the government considers “high risk” for “severe” Covid is so long that pretty much anyone could weasel into one of the categories. Who’s to say you didn’t just take up smoking? Or maybe you’ve been “physically inactive” recently.
Once someone gets a prescription, they can just go to a pharmacy, which are well-stocked with the drug.
But that’s a lot of work. Imagine how much lower vaccine uptake would be if people had to do all that just to get one.
It’s even worse to create a maze like that with Paxlovid, because it’s more time-sensitive than vaccines. The 89% effectiveness rate requires that you take Paxlovid within five days of symptoms starting.
The above steps for getting a prescription also may not sound like that much work to someone with insurance, who uses the medical system regularly.
But 82 million Americans don’t even have a primary care doctor.
Think they’ll get a Paxlovid prescription rapidly?
Also, millions of additional people have a doctor, but will normally just wait and see if their illness passes, and may not know about Paxlovid. I know I didn’t call a doctor when I got Covid back in 2020.
Why sitting on shelves? Reason 2: Media & Politics
The problem is compounded by the media, which has not covered Paxlovid much. I bet you haven’t seen any headlines blaring: “FINALLY, an 89% successful cure to Covid is available! The crisis as we know it is over!”
In December, only 52% of Americans had heard anything about the drug, and there’s also been little media coverage since then.
If everyone knew we had an effective treatment for Covid, death rates would fall faster.
Why the massive lack of information? I suspect it’s a perfect storm of political problems:
— The media (and “the left” generally) are afraid to tout an effective treatment too much because they fear it might discourage people from vaccinating, masking, or taking other precautions.
— Many on the “the right” may also not feel the need to talk about Paxlovid, because they already believe that Covid is not a big deal, or that Ivermectin already is an effective treatment. The data are clear that Ivermectin does not work at all, by the way.
Is Paxlovid safe enough? Yes.
From the 89% success rate, it seems natural to conclude that Paxlovid should be handed out like candy to anyone who tests positive.
But let’s do some due diligence on that first.
Here’s what we know about safety.
The Paxlovid fact sheet for health care providers describes what the clinical study found:
The safety of PAXLOVID is based on data from … a Phase 2/3 randomized, placebo-controlled trial in non-hospitalized adult subjects with [Covid] …
2,224 symptomatic adult subjects 18 years of age and older who are at high risk of developing severe COVID-19 illness received at least one dose of either PAXLOVID (n=1,109) or placebo (n=1,115)…
The proportions of subjects who discontinued treatment due to an adverse event were 2% in the PAXLOVID group and 4% in the placebo group.
In other words, people with the placebo were MORE likely to stop taking Paxlovid (due to what they thought were side effects) than the people who were actually given Paxlovid.
This makes some sense, considering that these were people with Covid. The people given the placebo were surely experiencing negative effects from Covid, and clearly, they mistakenly attributed some of those negative effects to Paxlovid (which was actually a fake placebo.)
The fact that they were more likely to stop treatment than the group that actually got Paxlovid is in line with Paxlovid working to reduce Covid symptoms.
There were a few symptoms that were worse with Paxlovid. Specifically:
Adverse events (all grades regardless of causality) in the PAXLOVID group (≥1%) that occurred at a greater frequency … than in the placebo group were [loss/distortion of smell] (6% and <1%, respectively), diarrhea (3% and 2%), [high blood pressure] (1% and <1%), and [muscle aches] (1% and <1%).
So, it is possible that the drug makes smell loss more likely. All other adverse advents were pretty similar when compared to the placebo — or even better.
The British Medical Journal summarizes:
People in the antiviral group were less likely to have a serious adverse event (1.7% versus 6.6% in the placebo group) or to have discontinued the study because of an adverse event (2.1% versus 4.1%).
Side note on effectiveness of Paxlovid + Vaccine
As a side note, the Paxlovid trial was done on unvaccinated people.
The effectiveness could be less than 89% on vaccinated people — though since Paxlovid works by disabling the replication of the virus itself, it also stands to reason that it would remove 89% of whatever remaining low risk a vaccinated person has, as well (same goes for people with natural immunity.)
Big picture: The Covid crisis is MOSTLY over, even without Paxlovid
Deaths in the US are falling, but the impact of Covid is still significant. Here’s a graph of all deaths in the US1:
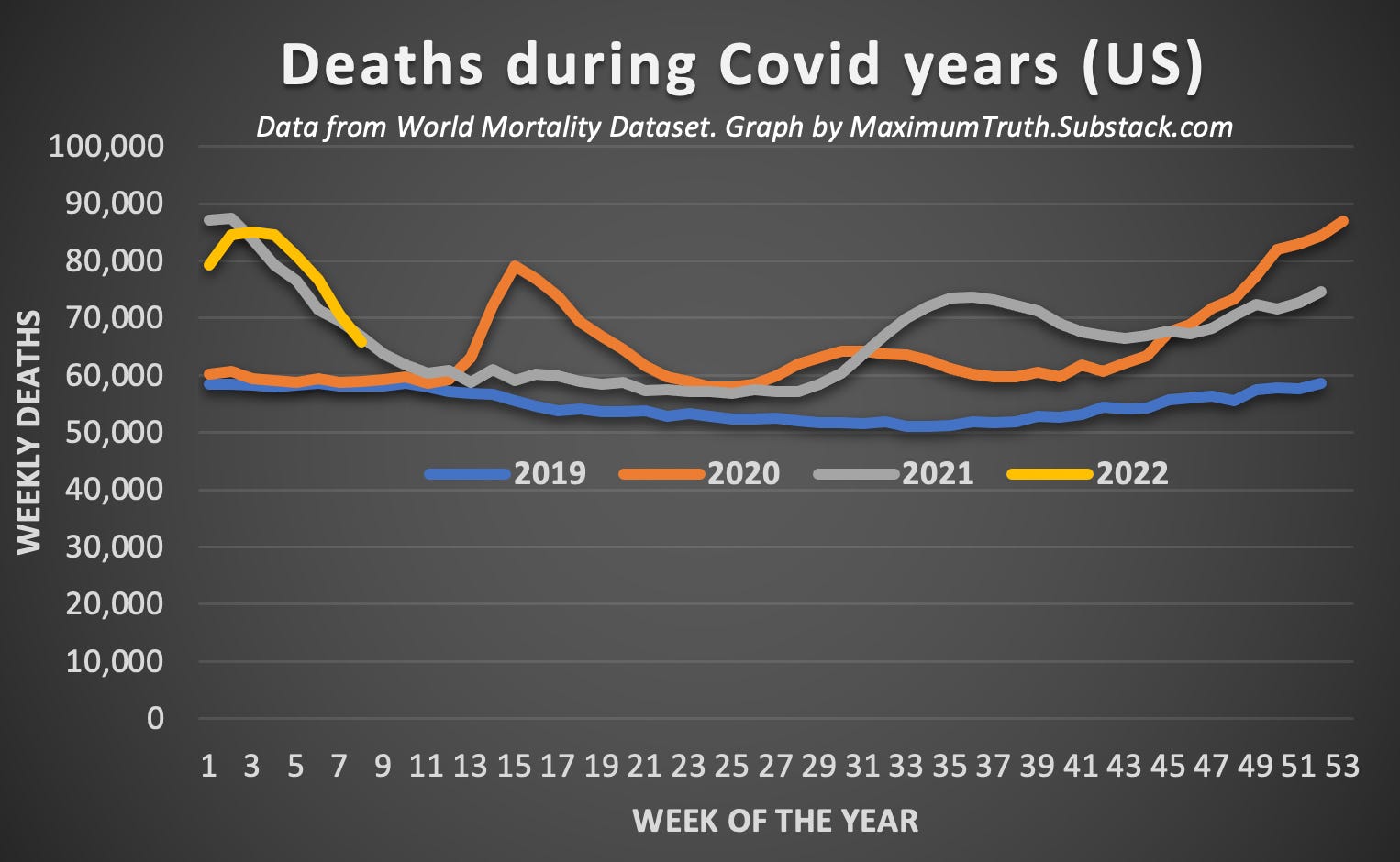
I use deaths from all causes to avoid any concerns about how Covid deaths are counted. The graph shows that Covid waves have been a major factor in total deaths — in some winter weeks, it increased total deaths by as much as 50%.
Deaths in 2022 are pointed in the right direction. The graph only goes through the end of February (as it takes a while before comprehensive mortality data is made available.) It’ll likely keep falling for a while, based on data for deaths specifically marked as Covid.
There’s other good news, too, such as the fact that in England, catching Covid is now just slightly less deadly than the flu. But it’s simultaneously true that Covid remains several times more contagious than the flu, and so is still several times more harmful to society.
The reduction in mortality is due to less-harmful variants, sky-high vaccination rates in the UK, as well as natural immunity. The UK government found that 98.8% of Brits now have antibodies to Covid:

I ran the numbers on the US, and it is well over 90% for adults. Below, in blue, are CDC data showing how many Americans in each age group got at least one dose of the vaccine. In orange is conservatively-estimated antibody prevalence (both from vaccines, and from Covid.)2
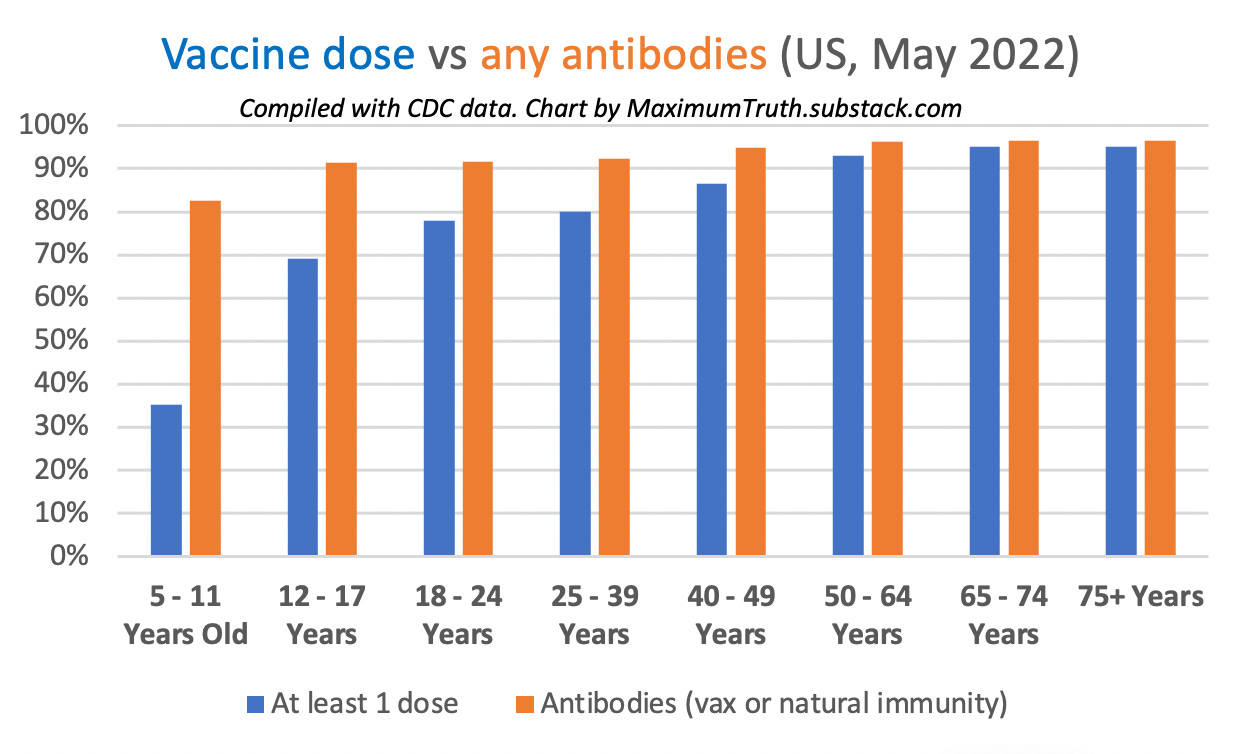
That high immunity is great, because having pre-existing antibodies reduces the chance of hospitalization and death enormously, by roughly 90%.
Conclusion: Government and media should report about Paxlovid more, and then get out of way
Covid’s negative impact is already mostly over thanks to vaccines, natural immunity, and variant changes. But it continues to kill far more people than we’d like — far more than the flu, or many other common causes of death.
Paxlovid is a treatment that actually works. It’s safe. And it’s under-used, because it’s over-regulated and the media ignore it.
More awareness that it exists would be a good start!
Beyond that, we should recognize that the Covid crisis is over.
It makes little sense to mask up, to demand vaccines and tests for travel, or to mandate anything in general — considering that Covid is here to stay and considering that the treatment situation is unlikely to improve much beyond what we have: a vaccine effective at preventing death, lots of natural immunity, and also an 89% effective treatment.
Instead of worrying about mask mandates, authorities should be making sure that everyone knows how to get this treatment that’s already available!
Authorities should also remove their regulatory roadblocks, and allow any adult with a positive Covid test to walk into a pharmacy and get lifesaving Covid treatment.
Note: FYI, OurWorldInData’s chart (which I was initially going to use here) is outdated. As of May 6 2022, it gives the wrong impression that deaths are already below the pre-pandemic baseline.
I instead got the latest data for my chart in this post directly from their source, the World Mortality Dataset: https://github.com/akarlinsky/world_mortality/blob/main/world_mortality.csv
I also left the last three database observations off the chart, after determining that deaths in the World Mortality Dataset historically tend to lag in the most recent entries (not all deaths have been reported yet.) The data in my chart should be close to final (but unfortunately, also only go to the end of February.)
To calculate this, I used the CDC’s vaccine data, and data from the CDC study on antibody prevalence here: https://www.cdc.gov/mmwr/volumes/71/wr/pdfs/mm7117e3-H.pdf
My graph assumes that non-vaccinated people got Covid at the same rate as the general population; in reality, it was probably higher (but we don’t know by how much) and as such the graph should be regarded as lower-bounds for antibody presence.
Good article. I see something else to think about. Using the % of people with antibodies, and info on the number of people vaccinated, and how well the vaccine worked, can you figure out how many people in the US have had covid? From that and the 1 million that are said to ahve died from it (but maybe use Excess deaths instead?), could we get a reliable death risk from covid?
Does Paxlovid treat Long COVID?
It seems pretty clear that the acute consequences of COVID are mild enough for healthy, fully vaccinated people that for most people it makes sense to go back to life as it was before the pandemic. But I've seen many estimates of long COVID suggesting its prevalence is concerningly high, and very little discussion of this from public health experts or authorities. (Zvi had a post on this in Feb - https://www.lesswrong.com/posts/mh3xapTix6fFtd3xM/the-long-long-covid-post - which reached conclusions similar to your own post on the subject. But there have been a couple of posts since then making claims to the contrary, which he hasn't engaged with:
https://www.lesswrong.com/posts/vSjiTrHkckTPrirhS/hard-evidence-that-mild-covid-cases-frequently-reduce
https://www.lesswrong.com/posts/emygKGXMNgnJxq3oM/your-risk-of-developing-long-covid-is-probably-high)