
A Lost Lesson of Covid: Ventilate!
Make the indoors more like the outdoors to prevent airborne diseases

Covid is over. It has joined the flu and the common cold as just another disease to put up with.
But the lessons from Covid are still useful. One is that transmission is virtually non-existent outside. Could that insight help us reduce disease prevalence in general?
I’d think so. The difference between outdoors and indoors mainly comes down to airflow and UV sunlight. So with enough fans blowing new air in, or with UV light, could indoor spaces become as safe as outdoor spaces?
I first heard of the notion from Alex Tabarrok at Marginal Revolution. He wrote:
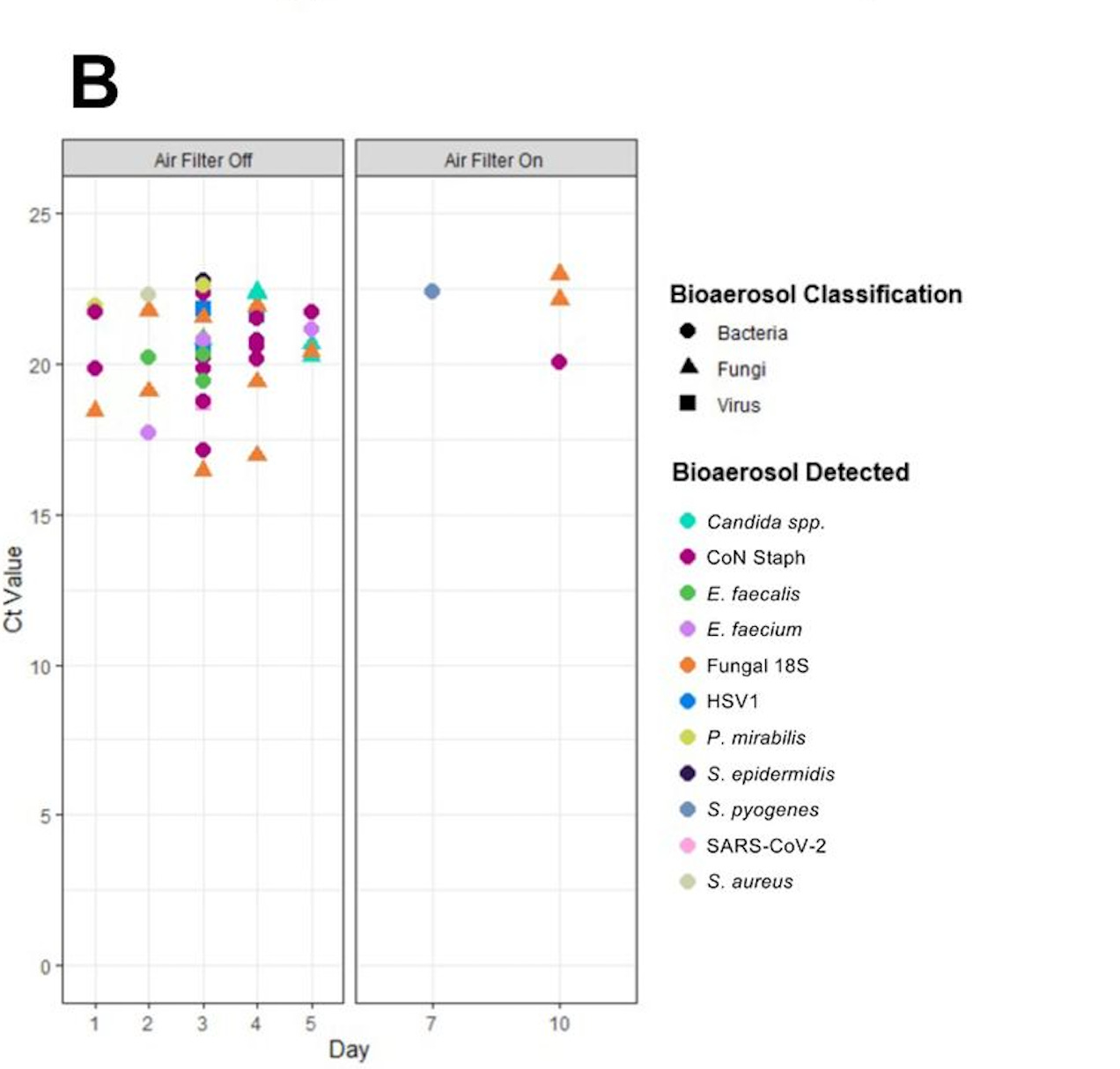
A recent paper … shows that air filtration and UV disinfection can greatly reduce SARS-COV-II in hospital wards. The authors installed portable air filters with UV disinfection on two COVID hospital wards in the UK … the portable filters and UV light … greatly reduced multiple viral, bacterial, and fungal pathogens.
Here’s the most relevant graph from the paper. The left panel shows pathogens in the air without filtration, and the right panel, with it:
If it’s so effective, why isn’t such filtration more common?
I figured cost was likely a big problem. But, digging into the study, the filter they tested in the ICU ward is not that expensive:

Certainly, it’s not expensive in a hospital system that sometimes charges patients that much for things like a single “routine nasal swab test” and for blood tests.
No good randomized, experimental studies have estimated the effect of air filtration on actually catching colds
The above study shows filtration and ventilation reduce disease particles in the air. That seems a good reason to think transmission would also be lower. But there aren’t good experimental studies actually testing that. A summary of studies on ventilation notes that:
ventilation [and] air cleaning devices … may have a role in reducing transmission ... However, the evidence was usually of low or very low quality …
One of the less-weak studies surveyed over 100 schools, and found:
Adjusting for county-level incidence, COVID-19 incidence was 37% lower in schools that required teachers and staff members to use masks, and 39% lower in schools that improved ventilation, compared with schools that did not use these prevention strategies.
Ventilation strategies associated with lower school incidence included … opening windows, opening doors, or using fans (35% lower incidence), or in combination with … (HEPA) filtration … 48% lower incidence.
The study wasn’t experimental/randomized, so there are likely confounding variables (for example, the schools that took these measures may have also taken un-measured precautions.) But basically, the best available (weak) evidence suggests that just opening windows is as good as making everyone mask up, and that adding an air filtration unit is better than that.
It is clear that Covid and the flu don’t spread much outside
A study in the Journal of Infectious Diseases from 2021 notes that:
the odds of indoor transmission was very high compared to outdoors (18.7 times; 95% confidence interval, 6.0–57.9).
So outdoor transmission is between 6 and 58 times less than indoors.
That seems plausible. I came around to the ultra-low risk of outdoor spread when the Black Lives Matter protests and riots first began, and health officials reversed their guidance against public gatherings (as long as the gatherings were about anti-racism.) While an insane policy, I was eager to see what would happen to Covid cases — would they spike, with everyone out breathing on each other in the streets? Over the following months, the data came in: Covid cases did NOT spike.
Studies on the flu are scarcer than for Covid, but there is evidence of reduced harm outdoors. The study mentioned above summarizes another:
Summers et al. conducted a historical analysis of a large outbreak of the 1918 influenza virus on a military troop ship in July 1918. The outbreak involved over 1000 of the 1,217 crew members and caused 68 deaths. Analysis of factors that might have contributed to mortality revealed a significant association between individuals who slept indoors, in cabins with bunks (mortality of 146.1/1,000 population), versus individuals who slept in hammocks in open-air areas (mortality of 34.1/1,000 population). This study is of particular interest because the duration of exposure and distance between individuals was held constant …
Cost of the common cold
This is an important question, as anyone who’s had a cold can relate to. But let’s quantify it anyway: The latest study I could find on the cost of the common cold put it at $40 billion in 2000. Adjusting for GDP growth, that would now be $107.83 billion.1
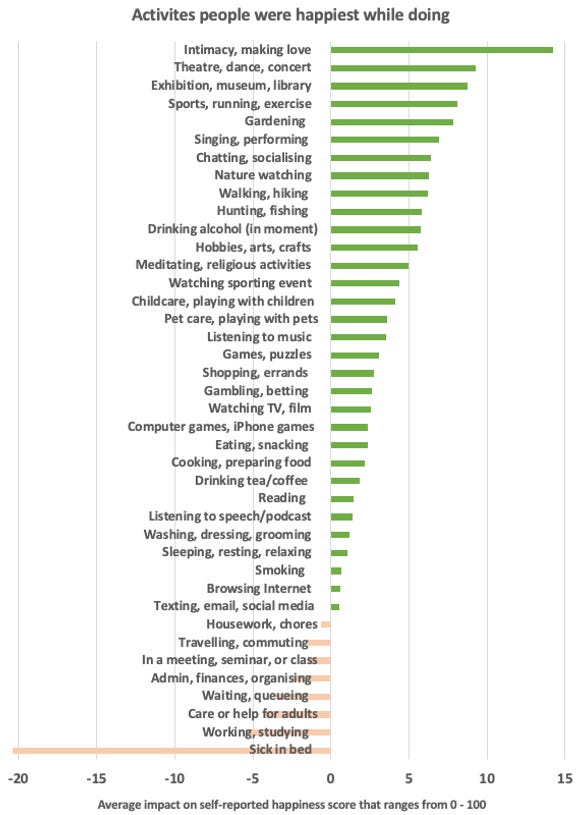
That’s just under half of 1% of total economic output. The effect on happiness is probably even more important, as the bottom of this graph cited in last week’s post suggests:
Why aren’t places doing more ventilation?
I think most people are just unaware of how helpful ventilation appears to be for preventing cold transmission.
Even if people are aware of the benefits, there may be a bit of a collective action problem. But step one is people actually valuing ventilation properly.
Before businesses, hospitals, etc, will pay money to set up good ventilation, their executives need to know that it works. It also helps if customer know, and can prefer to go places with ventilation.
People should also do more studies to confirm this, but it sure looks like it’s very effective, from what we know.
Conclusion: Covid taught us that being outdoors, or ventilating indoors, was great for preventing diseases. Let’s learn that lesson!
While society is waiting to catch up, there are things people can do as individuals:
Is someone coughing behind you on the airplane? Try turning on the overhead air vent to blow some of it away. Planes actually have excellent air filtration systems.
Seeing someone with a cold? Meet outside.
Is your Uber driver sneezing? Make sure a window is cracked open.
… etc.
Of course, fresh air is nice anyway, unlike masking — so this solution is really a win-win from all perspectives.
P.S.: regarding colds: Studies find that zinc lozenges reduce cold length and severity significantly, by a third. [Update: Commenter Milli notes that there is a small randomized trial showing no effect. Then again, a LessWrong poster notes that the trial used zinc lozenges mixed with “ … mannitol. And mannitol is one of the things mentioned by some studies as blocking zinc’s action.” Anyway, the published evidence is conflicted.] Apparently, zinc is toxic to bacteria, and useful for the immune system. Anecdotally, I’ve been taking them for 2 years whenever I get a cold, and they have improved things significantly for me. I think they’re even more effective when used preventatively before symptoms start.

(28225/10470)*40
> Before businesses, hospitals, etc, will pay money to set up good ventilation, their executives need to know that it works. It also helps if customer know, and can prefer to go places with ventilation.
In regard to restaurants and other places where people gather voluntarily, the businesses will pay money to set up good ventilation only if something forces them to. I gather that the cost is not insignificant -- the faster you turn over the air, the more you have to pay to heat/cool it. There have been sporadic press reports of retail businesses being strongly opposed to any legal standards for ventilation. And it's difficult for the patrons to judge whether a place has better ventilation or worse.
Re zinc lozenges: They likely don't work better than placebo.
https://bmjopen.bmj.com/content/10/1/e031662.abstract
Discussion on LessWrong: https://www.lesswrong.com/posts/5DKqK3hEzzBoGF47C/consider-taking-zinc-every-time-you-travel#cJFDzPYN6WtpdmTkS