
Defining mental Illness: Reconciling the views of Scott Alexander and Bryan Caplan
A theoretical model using "indifference curves" from economics

Note: This post is very abstract, and also inside-baseball. It tries to bring increased clarity to an existing debate among several rationalist bloggers. I advise skipping it if you don’t like very theoretical analysis.
Some of my favorite bloggers are having a lively debate about what constitutes a “mental illness.”
Scott Alexander (a psychiatrist) argues for a relatively conventional model, where someone who’s depressed, autistic, ADHD, etc, can be considered “mentally ill.” In less-clear-cut cases, it might come down to society’s values as to what counts as “illness”:
it’s a political question whether or not to classify any condition, including physical conditions, as illnesses. It’s just that the political question is usually very easy…
Bryan Caplan (an economist), in contrast, argues: “most so-called “mental illnesses” are not illnesses at all, but socially disapproved preferences.” So alcoholism can be re-framed as merely an extreme preference for drinking, ADHD can be re-framed as a preference for novel stimulus, and “anxiety” could be reframed as an unusual preference for avoiding danger.
I think they both make important points, but that Scott’s model is more fully correct. Here, I’d like to “economics-ify” Scott Alexander’s model a bit, which I think may help it translate to economists, and also force us to think a bit more rigorously:
Thinking like an economist: Spitting up preferences and constraints
Scott and Bryan have been at this debate for years now, and I wonder if some of their talking-past-each-other results from Bryan using an economist’s model of the world.
Below is an “indifference curve” that is taught in intermediate microeconomics classes. Has Scott seen these?
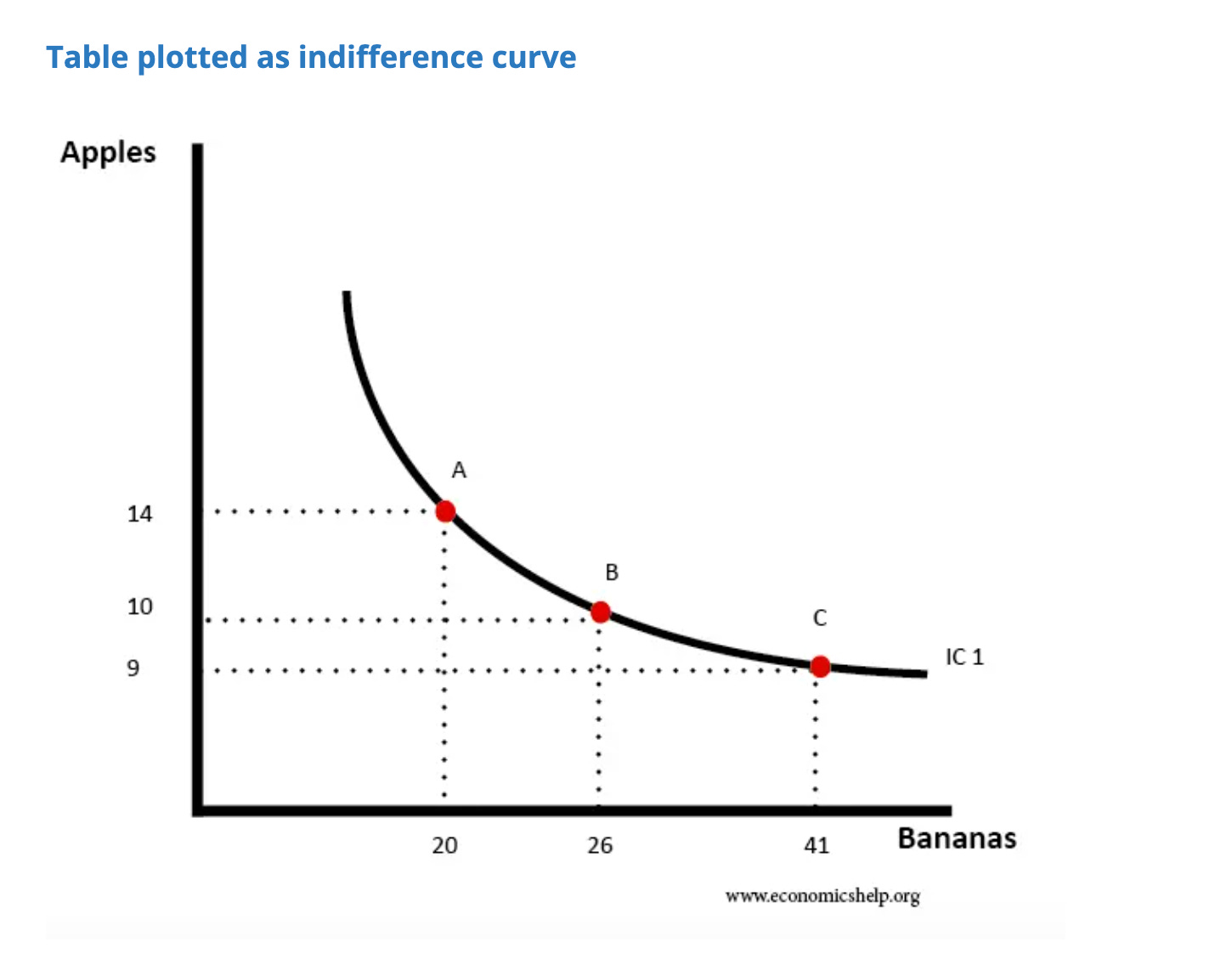
The idea of this “indifference curve” is to ask: what balance of apples and bananas would a consumer (for example, you) want?
The answer is more complicated than X apples and Y bananas. Actually, there are many different pairings of fruit that you’d be indifferent between.
In the hypothetical curve above, the consumer is indifferent between any set of coordinates along the black line. That means they would be equally happy to have 14 apples and 20 bananas (dot A) as to have 9 apples and 41 bananas (dot C).
What the consumer actually buys when he/she goes to store is then determined in conjunction with a second line, the budget constraint line:

When you combine the two lines, you get the amount actually purchased:

A person always has multiple indifference curves — the further-out indifference curves are strictly better. If prices rose, the consumer would have to buy less, and move down to a worse indifference curve, and be worse off.
In the above, we can see that this consumer bought 20 apples and 10 bananas, and was pretty happy.

If you change the prices, the budget constraint will shift:

All this corresponds to one example that Scott Alexander gives in his rebuttal to Caplan, in which Scott notes that you could think of a Coke-vs-Pepsi tradeoff in two ways:
Liking Pepsi more than Coke. You could think of this as a preference for drinking Pepsi over drinking Coke - or as an internal state marked by a strong repulsion to Coke plus a strong attraction to Pepsi.
But the economics worldview has a very clear way of categorizing this: someone’s preference for Pepsi is reflected in the shape of their indifference curve.
Scott’s says “internal state” and “strong repulsion”, but in this model, they seems to boil down again to just: preferences. They would both be modeled with an indifference curve.
Thinking like an economist: academic imperialism edition
Economists are famous for applying their models and statistical methods to subjects in all kinds of fields, with psychology and sociology being favorite targets.
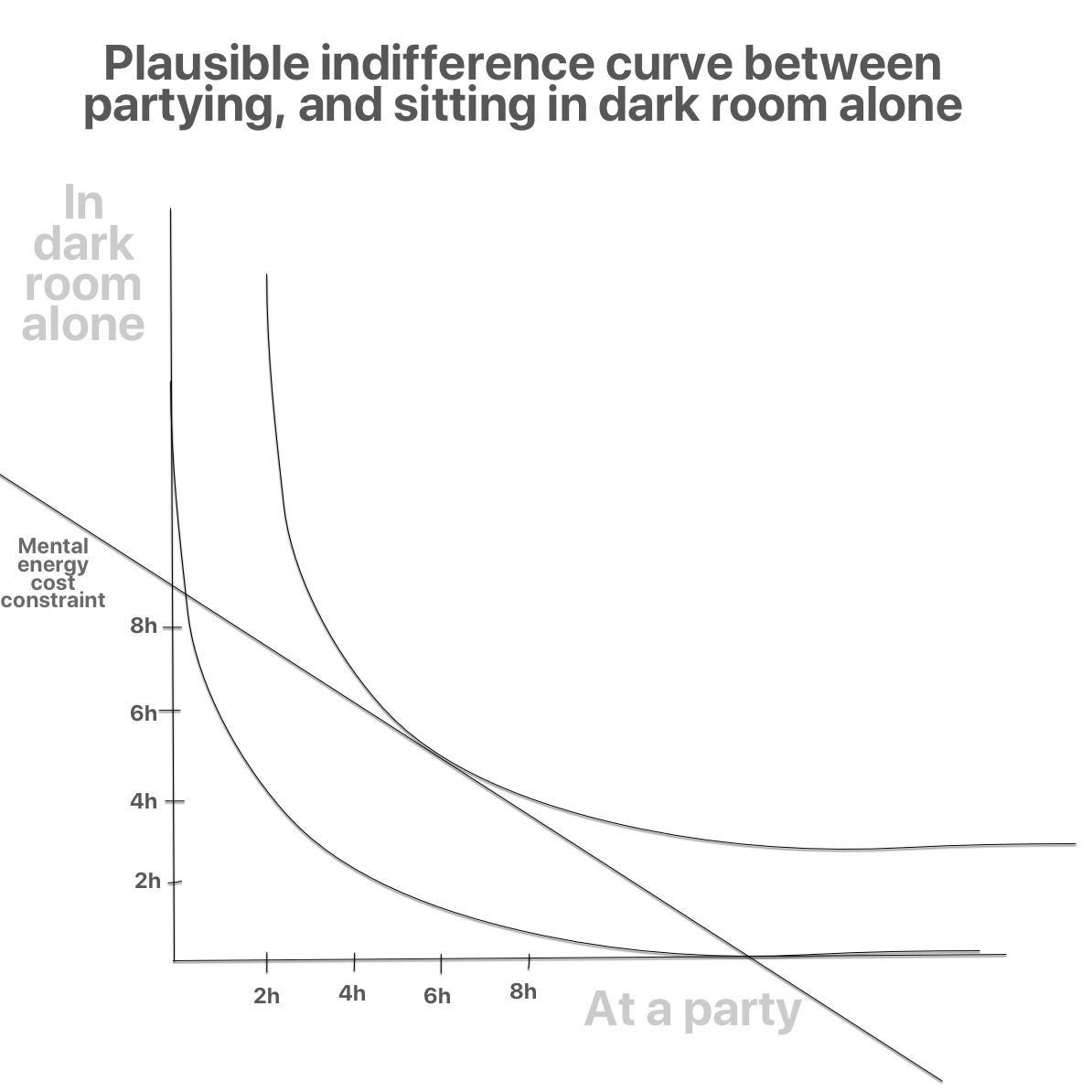
If we can model a tradeoff between apples and bananas, can’t we model, say, the tradeoff between going to parties or sitting alone? (Which is related to an example Scott brings up.)

The graphs show that the imaginary person is indifferent between, say, 6 hours alone plus 2 hours partying — or spending 2 hours alone plus 6 hours partying.
Partying, or being in dark room, doesn’t cost money. But those things do cost time, plus “mental energy”. We could consider those to be “cost constraints”:

So this individual chooses to spend nearly 4 hours at a party, and about 2 hours alone in a dark room.
Seems reasonable enough.
But now let’s say the person gets a migraine, per Scott’s example:
Consider a migraine. If we think like behaviorists, all we can really say about migraines is that someone locks themselves in a dark room, clutches their head, and says “oww oww oww” a lot.
In the model, the migraine adds a huge cost to partying, but the cost of sitting in a dark room doesn’t change much. So we get a new budget line like:

Now the model shows that the person will spend all day in a dark room, and zero time partying (where the blue and black lines intersect.)
Let’s say you now raise the cost of NOT partying to near infinity. To borrow Bryan Caplan’s hypothetical, imagine that someone held up a gun and required the person to party all day, despite the migraine.
Now the person’s cost constraint would look like:

Now the person spends all day at the party, despite the migraine.
My drawings oversimplify one thing for the sake of making the main point clear; in reality, you have many preference curves at different levels, and you prefer the further-out curves. So perhaps the original no-migrane curve would look like this:
Hitting that higher indifference curve means the person is more satisfied. The migraine, and then the gun, each moved the person to a much lower curve, making their life worse.
It follows that we could make the person’s life better by removing, first, the gun, and then the migraine. Controversial conclusion, to be sure…
But the important thing is that we now have this model for analyzing conditions.
When should a condition be part of the indifference curve, and when should it be in the budget constraint?
In the above situations, it’s obvious that a rise in the cost of bananas should be modeled as part of the cost constraint, and not as the preferences (indifference curves) themselves.
It seems clear that a migraine should be considered in the same light. After all, a migraine is transitory. It can occur due to all kinds of external triggers, like weather and drinking. It doesn’t seem to be “who you are” much more than a change in the price of bananas is “who you are.”
What about more complex conditions? Take depression, another of Scott’s examples:
Depression due to hypothyroidism. You could think of this as a preference for very low activity levels - or as an internal state of very low motivation and extreme fatigue.
So in the language of our model, what Scott is saying is that you could model this either as part of the indifference curve (preferences) OR as part of the constraint.
True, you COULD put it in either one. If you take the person’s hypothyroid-caused depression as it would be seen by an outside observer — you’d conclude: “oh, this person just really likes sitting in their room.”
Then, when the person spends all day sitting in their room, one could say “well they’re actually hitting the highest indifference curve available to them, so they’re doing fine!” This seems to be the “naive” economist approach. But a little theory about what is at the core of a person can enable us to improve on that.
Scott specified that the depression is due to hypothyroidism — which is typically caused “by the immune system attacking the thyroid gland and damaging it.” Surely the better way to model it is as part of the constraint. After all, the real person underneath their condition doesn’t want to sit in their room. It’s more that a broken body part is raising the cost of doing anything else.
Modeled that way, if you draw the graphs, it become immediately clear that treating the hypothyroidism/depression will allow a person to rise to higher indifference/preference curves. This is in line with common sense. The condition here isn’t even inherently a “mental illness”, but rather just “illness” that had an impact on mental function. It should obviously be treated.
But what if the depression were instead genetic, from birth? Where some abnormal piece of DNA caused a person’s brain to be wired in a way that produces low rewards for doing things?
In that case, it becomes harder to justify considering depression as a constraint. Instead, it seems it really is inherent to the person — and has to be modeled as the person’s preferences — their indifference curve. For a depressed person, that’ll mean indifference curves that lean toward lying in bed and doing nothing.
That might seem to support Caplan’s view, that mental conditions are merely preferences, EXCEPT that: the depressed person might also have a meta indifference curve to have new, non-depressed indifference curves.
Meta Indifference Curves
A genetically-depressed person can see that the people around them seem to have preference curves that appear better — and they’d love it if their doctor could give them a curve like the human median. We can imagine drawing a meta indifference curve, with goods/services on one axis, and changing one’s own indifference curve on another axis.

Considering this, I’d suggest a definition for “mental illness” such as: “any condition in which a person would willingly give up a lot to change their indifference curves to the median human indifference curves, after subtracting misguided social pressure.”
This is a bit similar to a point Arnold Kling made as well, about the validity of people who seek treatment for conditions.
Model note: Brain complexity, and time-slices
Under certain models of the self, the above isn’t fully comprehensible. Under the most simple model, if a person wants something (e.g., to lie in bed all day due to depression) it could be a contradiction for them to simultaneously want to want something else.
But because our brains are complex, containing both different conscious components, as well as ones below the level of conscious awareness — it is possible to want to want something else.
It becomes even more possible because each individual exists across different moments in time. In any moment, a depressed person might feel inclined to lie in bed all day — but across their life (including past and the likely future) they would prefer for their self across time to have indifference curves more like those of the typical human.
Social pressure caveat
In my suggested definition above, I added “after subtracting misguided social pressure”, which did not follow from anything discussed previously. But it is potentially important.
Homosexuality is the most obvious trait which used to be heavily stigmatized, and it was listed as an official mental illness. But increasingly, people have realized that it’s possible to be gay and live a normal, happy life. With modern technology, it’s also becoming increasingly possible for such couples to have biological children.
Yet if you had surveyed gay people in 1950, many of them would have probably paid to switch their orientation, if that could have been reliably done. Now that stigma is less, there are plenty who would not.
It seems wrong to call people “mentally ill” if they themselves are happy with their indifference curves.
Of course, ideally you would also not have social pressure against change one’s indifference curves.
Sometimes social pressure which is warranted — for example, there’s stigma against schizophrenia, partly because it can pose obvious danger to others, as one can verify with a quick trip to the NYC subway or any city in California.
In that case, someone with schizophrenia should ideally consider the legitimate outside pressure to be treated.
This is all about establishing a good theoretical definition. The reality, as Scott Alexander has written in many posts, is that our treatments are technologically primitive. Society doesn’t have reliable treatments for most mental conditions, and often the best therapies are only slightly effective in moving someone’s indifference curves, while containing their own risks.
I’m also under the strong impression that depression/anxiety medications are absurdly overprescribed in the United States, and generally shouldn’t be taken until one has first ensured adequate: exercise, sleep, and community/socializing. Usually those are the real problems, and humans are designed to not feel happy if we’re not getting them. Those problems should not be medicated away!
Where Caplan is right - borderline “mental illness” can often be good
While Caplan’s hard-line view on mental illness doesn’t seem to withstand the “meta” model above, I think a “soft” version of his view is correct: That mental illness is dramatically over-diagnosed in the United States.
In particular, there are lots of people with “conditions” like ADHD, mild autism, and OCD, who are wrongly medicalized and treated as if they were problems, when in fact they have different, valid indifference curves that they would not want to change. Or, even if they would want to change them in a world with perfect technology, the costs and side-effects of drugs far exceed the benefit.
That is particularly bad in schools in the United States, where 6 million kids have received an ADHD diagnosis, and over half of diagnoses are medicated. What are the odds that 10% of all kids are broken, vs. the school system being broken for them? If a kid can’t sit still, schools should encourage his/her non-sitting-still abilities and try teaching the student, say, oil field operation instead of algebra.
I know one journalist who says that ADHD has been good for his success — because his short attention span ensures that he’ll never bore his audience!
The benefits of mild autism are these days are now also widely appreciated in the tech/programming world, where such people are dramatically over-represented due to their ability to care about minutia and logic that would cause the median person to fall asleep.
No doubt OCD is also good for train schedulers, and much more.
There’s a relatively new word, “neurodivergent,” which aims to acknowledge that many people are quite different from the norm, while also not branding them with the negative “mentally ill.”
I think it’s great to have that positive word for indifference curves that differ greatly from the norm.
What should *society* designate as mental illness?
Now that we have a model and a definition, it’s worth going back to the question of public debate: what should society officially designate as mental illness?
It seems that society should only call something a disorder if the vast majority of people with the condition clearly see it as something they don’t want — after subtracting any needless social pressure.
The cost-benefit tradeoff is like:
Cost of designating something a “mental illness”: You harm the people with the condition who actually like their rare indifference curves.
Benefit of designating something a “mental illness”: You increase access to treatment for people who do want to change their indifference curves, or who should change them for society’s sake.
Based on this, one can see how different people come down differently, based on their own values/politics. Social conservatives argue that homosexuality and the trans movement are harmful to society for “undermining the traditional family unit.”
Emil Kirkegaard argues that exclusive homosexuality is a disorder on the grounds that it is evolutionarily un-adaptive.
But someone who doesn’t value evolutionary fitness or reproduction much, and who instead values individual self-realization more, will come to the opposite conclusion: That it should obviously not be considered a disorder, because doing so harms people who like their preferences.
It makes sense that, as society’s values have moved away from survival-and-reproduction focused concerns, towards more focus on individual autonomy and self-realization (as described by Robin Hanson’s farmer-vs-foragers model) we’ve seen a massive shift in how homosexuality and trans identities are perceived.
Values are subjective, so any given person’s view on what should be categorized as “mental illness” will naturally be different.
With that, we’re back to Scott’s point that:
it’s a political question whether or not to classify any condition, including physical conditions, as illnesses. It’s just that the political question is usually very easy…
Conclusion
Ultimately, Scott’s complex model seems closest to reality. Caplan also makes important points that I think can fit within that model, and Kirkegaard’s very un-PC arguments force us to think about what we value, and what we don’t.
Additionally, economic indifference curves can help bring clarity on how to think about preferences vs constraints.
I think this is essentially correct. However, it won't do anymore to convince Bryan than my shorter comments to the same effect because the real crux of the disagreement isn't over what you explained but about what 'mental illness' means.
Bryan gets himself into trouble because he tends to assume there are clear facts about the one right meaning of a word that reflect his intuitions about the principled distinctions in the neighborhood. In the case of mental illness, he seems committed to thinking that a mental illness somehow must mean a condition sufficient to excuse you (completely) from legal/moral responsibility for your actions and substitute in as an excuse where we'd accept a physical illness.
He doesn't seem willing to accept that the ascription of illness has multiple meanings depending on context ranging from: something we think should be fixed, to valid excuse for prescribing/subsidizing drugs, to a condition which justifies making allowances.
This is the same problem he runs into with his stuff on feminism. Sure, he's right that most people don't fully apply the definition the claim to accept about feminism being just the belief that genders deserve equal/fair treatment. But if he wasn't so stuck on the idea that words have a single true meaning he could just accept that (re) definition and make the same points rephrased as claims about how true feminism therefore requires equal focus on male mistreatment.
It's logically equivalent but he'd be a whole lot more likely to convince people like his daughter if he just accepted that many people simply don't want to have to say feminism is bad anymore than they want to say patriotism is and will change the meaning as needed to allow that.
Fine from an individual point of view, but weaker from the societal. You said:
..It makes sense that, as society’s values have moved away from survival-and-reproduction focused concerns, towards more focus on individual autonomy and self-realization (as described by Robin Hanson’s farmer-vs-foragers model) we’ve seen a massive shift in how homosexuality and trans identities are perceived....
Ignore the costs and risks to other people with a hand-wave towards 'individual autonomy and self-realization'? You also say:
...t seems wrong to call people “mentally ill” if they themselves are happy with their indifference curves....
But that ignores that there are whole public institutions dedicated to catching, holding and treating people, against their wills, for mental illnesses that the person does not want treated.
During the Covid panic, people were chased and caught by police simply for walking outdoors on a deserted beach. It was socially acceptable to arrest and detain people who might spread communicable diseases. Sometimes you can read of a tuberculosis+ person being arrested and forced into quarantine. So our tolerant, liberal US society is apparently schizophrenic about disease-spreading behaviors. Coughing on someone to spread disease is bad, but sex that spreads disease is just a choice?